Recurrent Shoulder Dislocation
The shoulder joint is the most mobile as well as the most unstable joint of the body. Hence the joint to undergo maximum dislocations in the body is the shoulder joint. This is due to the anatomy of the shoulder joint.
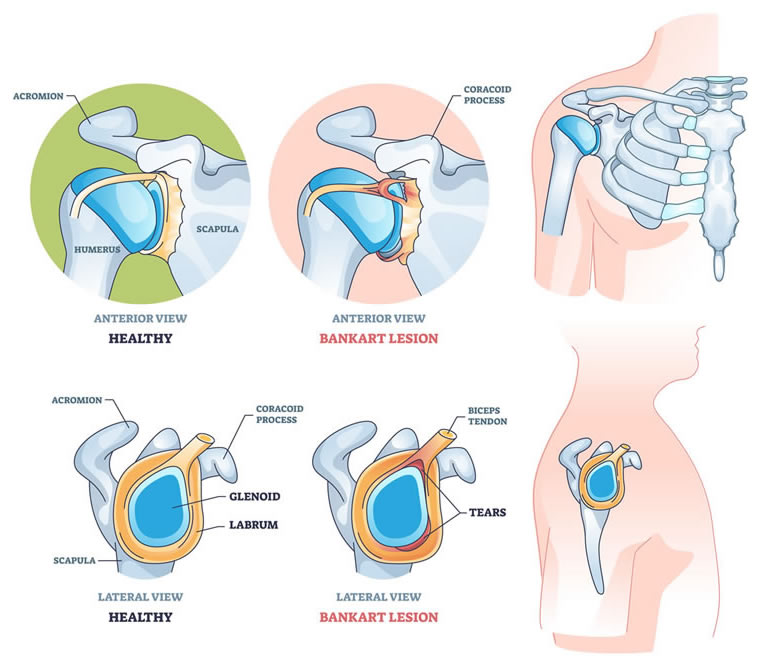
Bankart Lesion
The anatomy of the shoulder joint can be compared to a golf ball on a tee or a lemon on a spoon wherein the spoon is smaller and the lemon is bigger, thus making it a highly unstable joint. To stabilize this further the cup of the shoulder joint which is known as the glenoid on which the ball that is the head of the humerus rests is covered on all sides with specialized tissue which is called the labrum. This labrum serves 2 primary purposes. One it increases the surface area of the cup holding the ball making it more stable and second it has a vacuum like effect which holds the ball in place in its entire range of motion. The first time there is a shoulder dislocation there is a tear in the anteroinferior part of this labrum thereby making the shoulder prone to recurrent dislocation. The disruption between the Anterior Inferior Labrum And The Glenoid, as seen in traumatic anterior instability, was termed the “Essential Lesion” by bankart in 1938. Subsequently it has been dubbed the “Bankart Lesion.”
This disruption is critical in the development of recurrent instability because it serves as the anchor for the (inferior glenohumeral ligament) ighl, which is the primary static stabilizer against anterior and inferior humeral translation in abduction and external rotation.
Second, the concavity – compression effect formed through the combination of dynamic humeral head compression and the increased glenoid concavity by the labrum is disrupted.
If the ighl detaches with a small piece of avulsed glenoid, the lesion is called a Bony Bankart.
A bony bankart lesion can also be a “Shear” fracture.
Bankart Repair
A bankart repair is a surgery wherein the avulsed labrum is reattached back to the glenoid with the help of suture anchors thereby helping the labrum to perform its functions that is increase the surface area and hold the humeral head in place by its concavity-compression effect. A well-done bankart repair can produce good results in excess of 90% of cases. That does not translate into 90% success rate of bankart repair. Most often it means that other associated injuries have been missed. Bankarts repair surgery is most commonly performed arthroscopically. The advantage of arthroscopic technique is its ability to recognize associated injuries like hill-sachs, posterior and superior labral and rotator cuff tears. In addition, these could be addressed arthroscopically simultaneously.
It is often combined with another procedure called remplissage wherein the bony defect in the humeral head is filled up with infraspinatous muscle thereby reducing the range of motion and not allowing the humeral head defect to engage.
Most often large glenoid bone defects are the cause of failure. In properly selected cases, results are highly gratifying. In those patients who have large glenoid defects, open latarjet procedure is the treatment of choice.
Postoperative Rehabilitation
- Wrist and elbow rom exercises are started on the same day. A squeezing ball is given in the hand for patient to continuously exercise hand muscles.
- Gentle pendulum and scapular strengthening exercises are started on day one.
- All movements are allowed as tolerated except er. External rotation is restricted to neutral, 0 degree, for first 3 weeks till subscapularis heals. Resisted internal rotation is not allowed for 6 weeks for the same reason.
- Full rom (except er) is aimed by 3–4 weeks. Normal external rotation is achieved by 6–8 weeks.
- Rotator cuff strengthening is started at 6 weeks.
Arthroscopic Bankart Repair
Arthroscopic repair of bankart lesion is fast replacing its open counterpart as the procedure of choice in all but handful of exceptions.
In pure soft tissue lesions, where significant bone loss is not expected, results of arthroscopic repair are comparable to open repair. As subscapularis is not breached, faster functional recovery is seen.
Postoperative Management
- The patient’s shoulder is protected in an abduction splint for 6 weeks with no active shoulder use during this time.
- Passive range-of-motion exercises, including forward flexion and external rotation stretching, can be started within the first 6 weeks of surgery based on surgeon preference.
- At 6 weeks, active shoulder use is allowed and range of motion stretching is advanced to active exercises in all planes.
- Strengthening is started 3 months after surgery, with a return to contact activities at 5 to 6 months postoperatively
To know more kindly contact the best orthopaedic surgeon Dr. Rahul Modi for further queries.
This surgery is frequently performed by the best orthopaedic surgeon Dr. Rahul Modi for treating Bankart Repair.