Clavicle Fracture
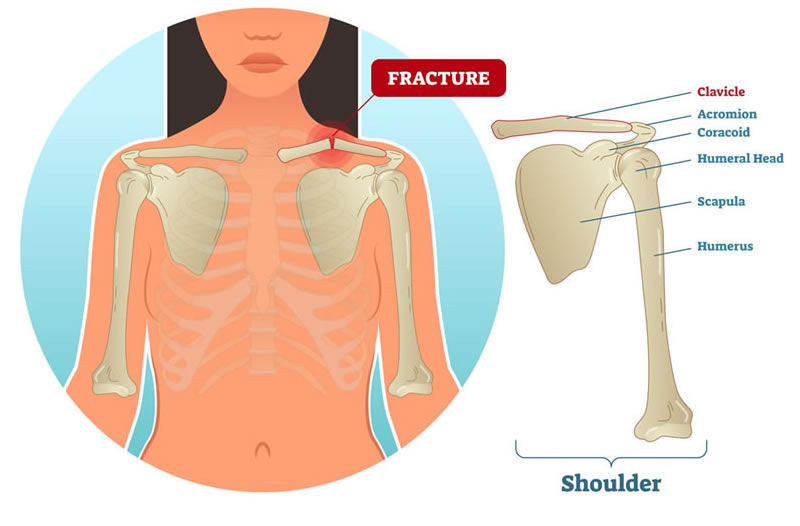
Shoulder Fracture
Clavicle, Humerus and Scapula are the bones involved in formation of Shoulder Joint.
Mechanism Of Injury
- Direct:
Due to fall on the point of the shoulder. This is the most common mode of injury accounting for 91 percent of the cases. - Direct Trauma:
Direct trauma over the clavicle due to RTA, direct injury, etc. accounts for 8 percent of the cases. - Indirect fall on the outstretched hands accounts for 1 percent of the cases.
Sites Of Fracture
- Eighty-five percent of the fracture clavicle occurs at the junction of middle and outer third
- One percent at the medial end of the clavicle (5%)
- Lateral end fracture is uncommon (About 10%) (Distal 1/3rd).
Sites Of Fracture
The patient presents with pain, swelling, deformity and inability to raise the shoulder. Rarely, the patient may present with pseudo-paralysis of the affected arm.
Radiographs
The following views are recommended: Routine AP view of the clavicle
Principles Of Treatment
Conservative Methods
This is the treatment of choice in fracture clavicle and consists of the following methods:
- Cuff and collar sling for undisplaced fractures.
- Strapping of the fracture site after reduction of the fracture by elevating the arm and bracing the shoulder upwards and backwards gives good results in both children and adults.
- Figure of ‘8’ is popularly used and it acts by retracting the shoulder girdle, minimizes the overlap and allows more anatomical healing.
Surgery
- Intramedullary fixation with tens nail.
- Open reduction and internal fixation with rigid plate and screw.
Indications
Open fractures, injury to neurovascular bundle, if the fracture is threatening to penetrate the skin, nonunion, fracture near acromioclavicular joint, floating shoulder, soft tissue interposition and displaced epiphysis in children.
More Specific Indications for Open Reduction and Internal Fixation of Fracture Clavicle
- Shortening or distraction of fragments for more than 2 cm.
- More than 100 percent displacement or fragmentation.
- Bilateral fractures.
Complications of Fracture Clavicle
Injury to important nerves and vessels, mal-union (the fracture unites in a non-anatomical position) and rarely non-union.
Proximal Humeral Fractures
This is common in elderly patients and it accounts for 4 to 5 percent of all fractures. It is more common in elderly females due to osteoporosis.
Mechanism
- Fall on the outstretched hands is the classical history.
- Blow on the lateral side of the arm is the other mode of injury.
It can be classified as,
Undisplaced And Displaced Fractures.
Displaced fractures can be further categorised into number of fracture fragments.
A two-part fracture is where one segment is displaced in relation to the other.
A three-part fracture is where two segments are displaced in relation to the other two.
A four-part fracture where all four major segments are displaced.
These above fractures when associated either with anterior dislocation or with posterior dislocation of shoulder are called two-part fracture dislocation, three-part fracture dislocation, etc.
Clinical Features
The patient complains of pain, swelling and other features of fractures. Movements of the shoulder joint are grossly restricted.
Investigations
- Plain X-rays of the shoulder: Trauma series consists of AP, lateral, and axillary view of shoulder joint in scapular plane.
- CT scan helps to study the fracture lines with greater accuracy.
Management
Non-operative Treatment Indications
- Undisplaced Fractures
- Surgical Neck Fractures
- Poor Health
- Poor Surgical Risks
- Very Old Patients
Conservative treatment consists of rest, NSAIDs, sling, ice and heat therapy in the initial stages.
Universal shoulder immobilizers, arm sling pouch, U–slab and rarely U–cast may be required in fractures with minimal displacement.
Operative Treatment
Rigid internal fixation of displaced fracture of the proximal humerus in older patients with a open reduction and PHILOS plate fixation is the gold standard treatment for treating displaced proximal humerus fractures and this provides sufficient primary stability to allow early functional treatment.
Restoration of anatomy and biomechanics may contribute to a good functional outcome when compared with alternative methods of fixation or conservative methods.
Regardless of age, they advocate primary open reduction and rigid internal fixation for a 3- or 4-part fracture. This depends upon whether the injury is two part, three-part, etc. or is just a plain fracture or fracture associated with dislocation.
Highly communited part 4 fracture needs prosthetic replacement with either a hemiarthrosplasty like a Neer’s prosthesis or a Reverse Shoulder Replacement surgery.
Complications
- Joint stiffness is due to periarticular fibrosis.
- Malunion is due to the varying muscle forces.
- Collapse of fracture fragments.
- Avascular necrosis is seen in fracture of the anatomical neck.
- Nonunion of surgical neck.
- Myositis ossificans due to vigorous massage and treatment.
Fracture of the Scapula
Scapula is a flat bone thickly covered by muscles.
Incidence
It is a rare injury.
- 3 to 5 percent of all shoulder girdle injuries.
- 0.4 to 1 percent of all fractures.
- Mean age is 35 to 45 years.
Functions
- Stabilizes the upper extremity against the thorax.
- Links the upper extremity to the glenoid.
Mechanism of Injury
- Direct Blow — Fall of a heavy object on the shoulder blade.
- Axial loading on the outstretched hands.
Classification (Thompson’s)
- Type I: Coracoid, acromion and small fractures of the body.
- Type II: The glenoid and neck fractures.
- Type III: Body fractures major.
Clinical Features
The patient complains of pain and swelling, arm is held adducted to the sides of the chest, all movements of the shoulder, especially abductions, are painful, may be associated rarely with pneumothorax and inability to elevate the arms may give a feeling of pseudo-rupture of the rotator cuff.
Radiographs
A true scapular AP view and a true lateral view (axillary view) helps to make the diagnosis. Sometimes a CT scan is also required.
Treatment
- Nonoperative Methods: Undisplaced scapular fractures may be treated conservatively with rest, sling, strap, etc.
- Operative Methods: Displaced fractures need open reduction and internal fixation with K-wires, screws and plates.
To know more kindly contact the best orthopaedic surgeon Dr. Rahul Modi for further queries.
This surgery is frequently performed by the best orthopaedic surgeon Dr. Rahul Modi for treating Shoulder Fracture.